Share this
by HEPACART on Jun 22, 2026

For an ambulatory surgery center, five minutes rarely feels like the whole problem.
It feels like a small delay between cases. A room that is almost ready. A containment setup that took slightly longer than expected. A facilities check that had to be repeated. An air change calculation that was not confirmed until the team was already waiting.
But in an ASC, five minutes does not stay five minutes for long.
ASCs operate on a throughput-driven model where operating room utilization, case volume, physician schedules, staffing, and reimbursement all sit tightly together. CMS maintains ASC payment rates and covered procedure files because reimbursement is tied to procedure-level payment structures, not broad inpatient revenue streams. That means lost capacity can quickly become a financial issue, not just an operational inconvenience.
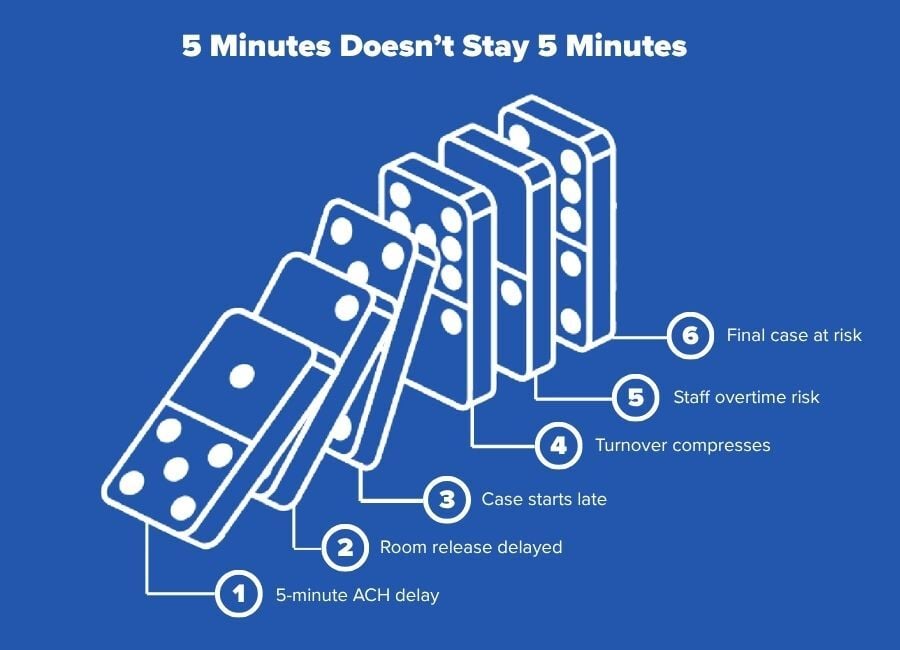
When air changes lag after construction, renovation, maintenance, turnover, or containment-related work, the delay can move through the day like a chain reaction. One room waits. One surgeon waits. One case starts late. The next case has less buffer. By the end of the day, that small airflow delay may contribute to overtime, rescheduling, frustrated physicians, or a case that no longer fits.
That is why ASC leaders should not only ask, “How do we calculate air changes per hour?”
They should also ask, “What does it cost when we do not know the answer fast enough?”
Why Air Changes Matter in an ASC Operating Room
Air changes per hour, often shortened to ACH, measures how many times the air volume in a room is replaced or filtered in one hour. In simple terms, ACH helps facilities, infection prevention, and construction teams understand whether the air control plan is moving enough air for the room size and use case.
For healthcare environments, ventilation is not just a comfort issue. ANSI/ASHRAE/ASHE Standard 170 is the healthcare ventilation standard used to define minimum requirements for healthcare facility ventilation. The 2025 edition continues to address healthcare facility ventilation requirements, outpatient spaces, and ventilation during construction.
Operating rooms are especially sensitive because air movement supports contamination control, pressure relationships, filtration, and protection of the surgical field. ASHE notes that ASHRAE 170 requires operating rooms to have a minimum of 20 air changes per hour, with requirements reestablished when the room becomes occupied after an allowed unoccupied setback.
For an ASC, this matters because OR time is revenue time. Airflow uncertainty does not just affect a mechanical system. It affects whether the room can be confidently released for the next case.
How to Calculate Air Changes Per Hour
The basic ACH formula is:
ACH = (CFM × 60) ÷ room volume
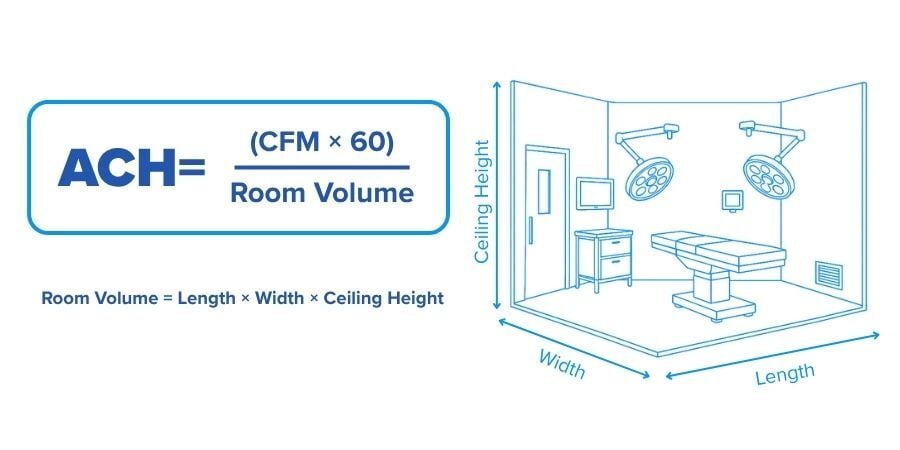
Where:
- CFM means cubic feet per minute of airflow
- 60 converts minutes to hours
- Room volume means length × width × ceiling height in cubic feet
For example, if an OR or procedure room is 20 feet long, 20 feet wide, and 10 feet high, the room volume is 4,000 cubic feet. If the system is delivering 1,200 CFM:
ACH = (1,200 × 60) ÷ 4,000
ACH = 18
That room would be receiving 18 air changes per hour based on those inputs.
This is why searches like “air changes per hour calculator,” “ACH formula,” “CFM calculator,” “ACH to CFM,” and “air change rate formula” matter. The math itself is not complicated. The operational problem is that the numbers are often needed quickly, in the middle of a live clinical schedule, with multiple teams waiting on the answer.
For a faster way to calculate air changes per hour, use the HEPACART® calculator here: Calculate Air Changes Per Hour
The Cost Breakdown: What 5 Minutes Really Means
Five minutes of OR downtime can show up in several different cost categories at once. Some are direct and easy to see. Others are indirect, but still painful.
AORN has reported that a 2018 study found the mean cost of one minute of OR time was approximately $36 to $37, with some estimates rising to $60 or even $100 depending on what is included. Another literature review estimated the mean cost of one minute of OR time at $46.04, adjusted to 2022 dollars.
Those numbers should not be treated as a universal ASC revenue figure. Case mix, payer contracts, staffing model, specialty, and local cost structure all matter. But they are useful for showing why “just five minutes” deserves attention.
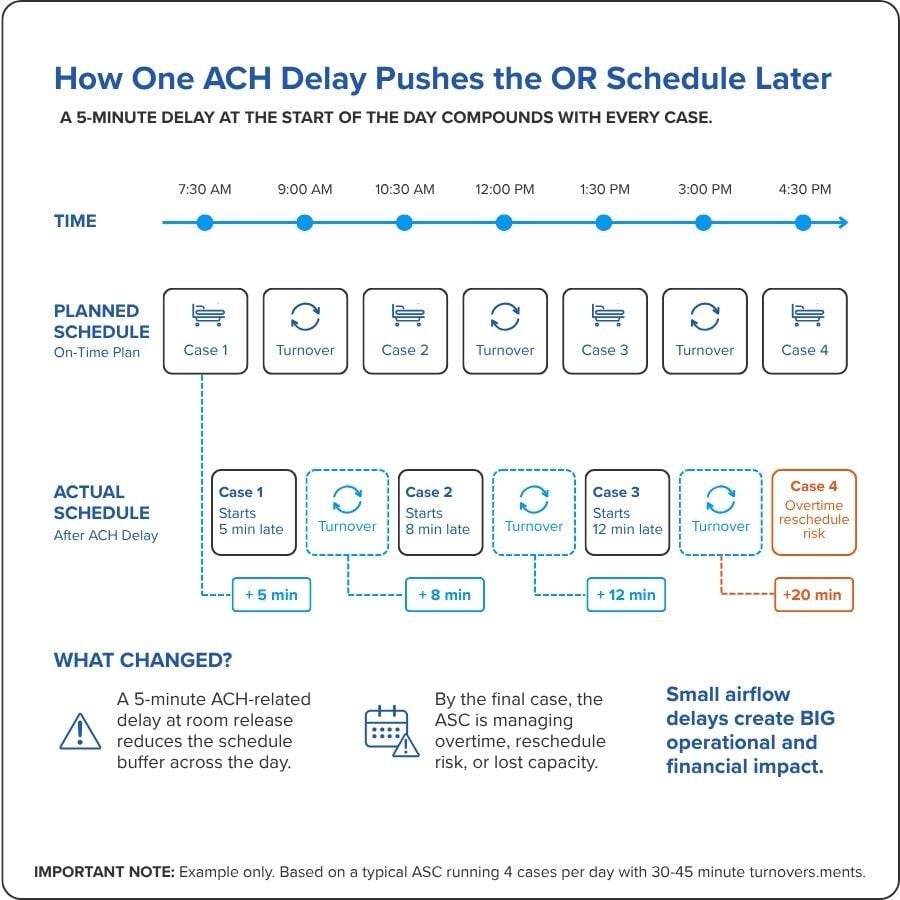
Example: 5 Minutes Across a Single OR Day
 This is only the OR time calculation. It does not include the potential revenue impact of a canceled case, rescheduled patient, physician dissatisfaction, staff overtime, or reputational strain if delays become a pattern.
This is only the OR time calculation. It does not include the potential revenue impact of a canceled case, rescheduled patient, physician dissatisfaction, staff overtime, or reputational strain if delays become a pattern.
In an ASC, the bigger risk is not always the five-minute delay itself. It is the loss of schedule control.
Where Air Change Delays Usually Enter the Day
Air changes can lag for several reasons, especially during renovation, maintenance, or phased construction in active clinical spaces.
 Common sources include:
Common sources include:
- A negative air machine is undersized for the room volume
- The team estimates CFM instead of confirming it
- Room dimensions are not available when the work starts
- Filters are loaded and airflow has dropped
- Containment setup changes the effective room volume
- Temporary barriers, anterooms, or work zones alter airflow paths
- Teams wait until turnover to confirm whether the air change rate is sufficient
CDC guidance for healthcare construction and renovation emphasizes educating construction teams and healthcare staff about airborne infection risks during construction activity and methods to control dissemination of fungal spores. That matters because a delayed air change calculation is not just a facilities inconvenience. It can become an infection control confidence issue.
The ASC question is practical: can your team verify airflow fast enough to avoid delaying scheduled procedures?
Why Small Delays Compound in ASCs
Hospitals can absorb some inefficiency through larger staffing pools, broader room capacity, and multiple revenue streams. ASCs usually have less slack. Their schedules are built around high utilization, efficient turnover, and predictable case flow.
AORN has highlighted how first-case delays can become severe in ASCs. In one AORN Journal case study discussed by AORN, an ASC had a first-case on-time start rate drop to 14%, with 156 out of 180 first surgical cases starting late during a four-month period.
That example is not specifically about ACH, but it shows the larger point: once schedule reliability breaks down, the issue becomes bigger than one room or one process. Delays become a system problem.
When air changes lag, the day can be affected in five ways.
1. The first delay eats the buffer
Most OR schedules have some buffer, but not much. If airflow verification takes five extra minutes after turnover or construction-related work, the schedule absorbs it once. The problem starts when the same delay happens again.
2. Staff time becomes waiting time
Nurses, techs, anesthesia, facilities, and environmental services may all be ready, but the room is not. The labor cost continues even when the room is waiting on air.
3. The surgeon schedule tightens
Physician satisfaction is a major ASC performance factor. If cases start late because a room is waiting on air change verification, the issue can affect surgeon confidence in the facility’s operational control.
4. Patient flow becomes less predictable
Late starts affect pre-op, recovery, discharge timing, family communication, and room availability. A small OR delay can create visible front-stage disruption.
5. The last case becomes vulnerable
The most expensive delay may not be the five minutes in the morning. It may be the case at the end of the day that no longer fits without overtime, staff pushback, or rescheduling.
The Hidden Cost Categories Behind ACH Delays
A cost breakdown should include more than the OR minute calculation. For ASC leaders, the financial impact usually sits across several categories.
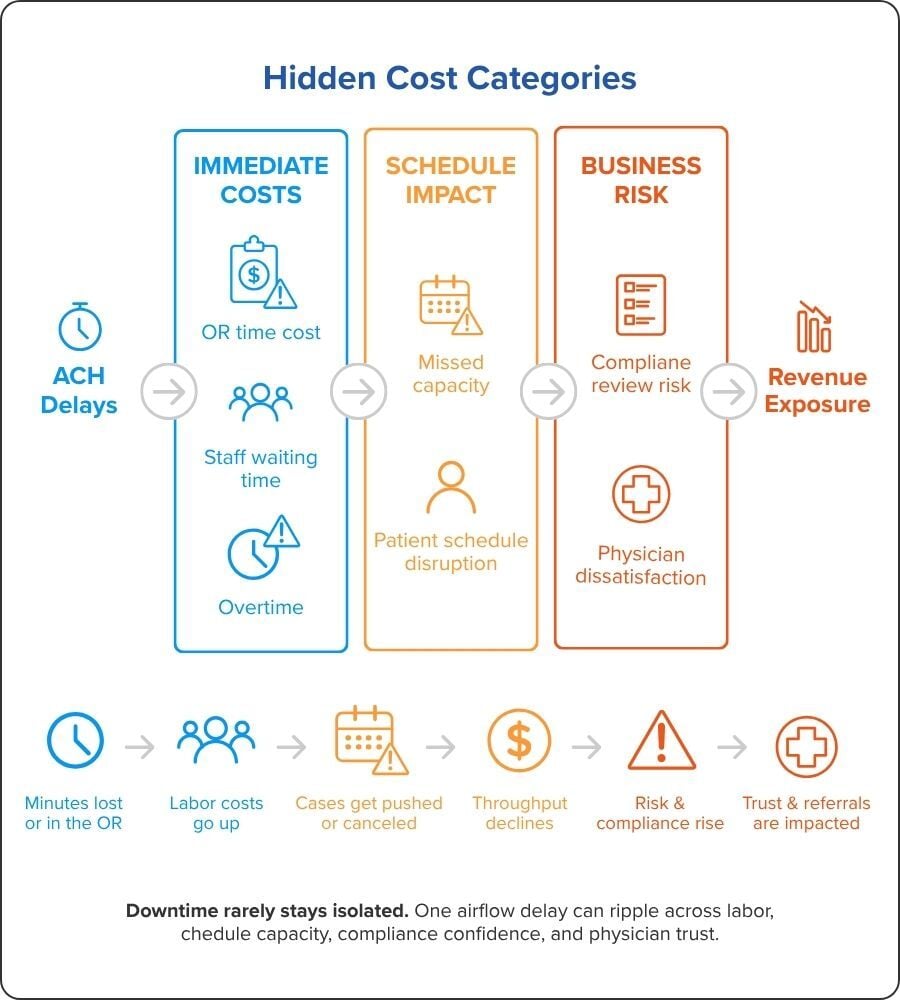
Direct OR time cost
This is the simplest category. It estimates the value of OR time lost when a room is delayed.
Use this formula:
Lost OR time exposure = delay minutes × estimated OR cost per minute
If you use $46 per minute as a planning estimate, a 5-minute delay equals $230 in OR time exposure. Across multiple rooms and turnovers, that number scales quickly.
Staff labor cost
The room may be idle, but the team is still on the clock. Delayed air changes may affect:
- Circulating nurse time
- Scrub tech time
- Anesthesia time
- Environmental services time
- Facilities or maintenance time
- Construction or contractor time
Even when the delay does not cancel a case, it can convert productive labor into waiting labor.
Overtime and extended day cost
If delays stack up, the final cases may push beyond the planned schedule. That can create overtime, late discharge pressure, and staff satisfaction problems.
The financial issue here is not only added payroll. It is the loss of predictability. Once teams expect the day to run late, morale and retention can become part of the operational cost.
Missed case capacity
This is where the economic impact becomes more serious. If recurring delays reduce the number of cases an ASC can complete, the cost moves from “lost minutes” to “lost case opportunity.”
That calculation depends on specialty, payer mix, contract terms, and procedure volume. CMS maintains ASC payment information by covered procedures and payment rates, which reinforces that case-level reimbursement is variable and procedure-specific.
A simple way to model this internally:
Missed capacity exposure = number of cases delayed or canceled × average net revenue per case
That number will usually matter more than the direct cost of a few minutes.
Compliance and infection prevention risk
If air changes are not verified or containment performance is unclear, the risk is not purely financial. It can trigger review from infection prevention, clinical leadership, accreditation teams, or external authorities.
For ASCs, that matters because downtime is expensive, but a compliance issue can be worse. It can affect patient safety, accreditation confidence, physician trust, and referral relationships.
Why “Close Enough” Airflow Planning Creates Risk
Some teams rely on estimates because they have done similar jobs before. That may work until conditions change.
A room may have a different ceiling height. A temporary containment setup may change the volume. A HEPA filter may restrict airflow as it loads. A negative air machine may deliver less effective CFM than expected under real conditions. A phased project may require a different pressure relationship than the last project.
This is why an air change calculator is not just a math convenience. It is a decision support tool.
To calculate air changes per hour correctly, teams need:
- Room length
- Room width
- Ceiling height
- Confirmed CFM
- The target ACH for the space or work condition
- Clear understanding of whether air is supplied, exhausted, filtered, or recirculated
- Alignment with applicable code, facility policy, ICRA expectations, and AHJ requirements
ASHRAE/ASHE guidance also notes that authorities having jurisdiction may adopt and enforce different editions of Standard 170, so facilities should confirm which edition applies to their organization.
That is an important point. The calculator helps with the math. It does not replace facility standards, engineering review, infection prevention approval, or applicable code requirements.
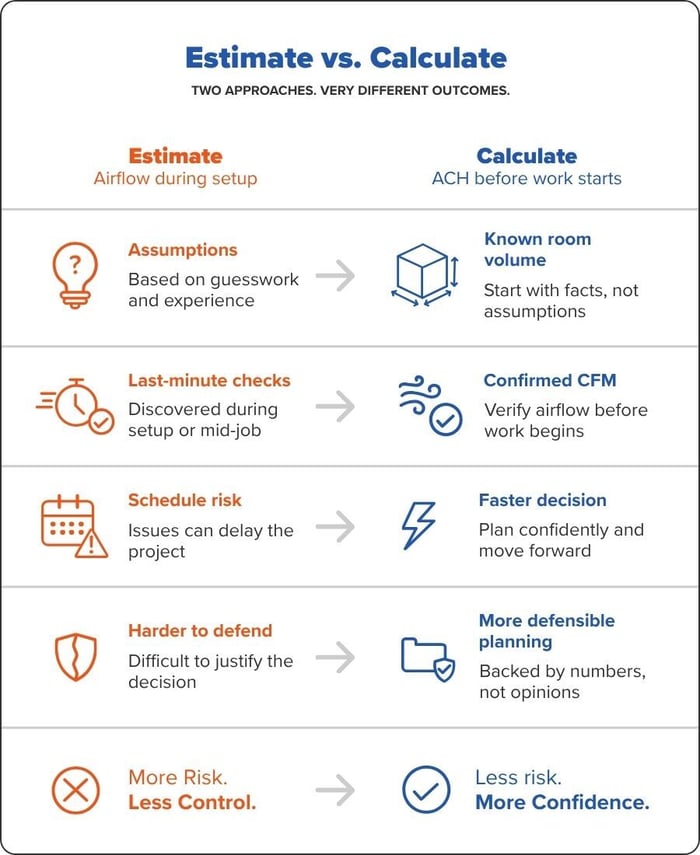
Comparing Two ASC Approaches to Air Change Planning
How to Reduce Downtime When Air Changes Are Part of the Work
ASC teams do not need more complexity. They need a repeatable process that helps facilities, infection prevention, and construction teams make faster decisions.
Step 1: Measure the room before the work starts
Do not wait until turnover or the morning of construction activity to collect room dimensions. Capture length, width, and ceiling height during planning.
Step 2: Confirm equipment CFM under real conditions
Equipment labels are a starting point, not the whole answer. Filters, ducting, containment layout, and static pressure can affect performance.
Step 3: Calculate ACH before the schedule is exposed
Use an air changes per hour calculator before the room needs to be released. This gives the team time to adjust equipment, airflow, or phasing without holding up cases.
Step 4: Document the expected target
Tie the calculation to the facility standard, project requirement, ICRA plan, or infection prevention direction. This makes the decision easier to defend.
Step 5: Recalculate when the setup changes
If the containment footprint changes, the room changes, or equipment changes, the ACH calculation should be revisited.
Common Questions About ACH and OR Downtime
What is the easiest way to calculate air changes per hour?
The easiest way is to use the formula ACH = (CFM × 60) ÷ room volume. Room volume is calculated by multiplying length, width, and ceiling height. A calculator can reduce errors and speed up the process when teams need an answer quickly.
What is the difference between ACH and CFM?
CFM measures airflow volume per minute. ACH measures how many times the air in a room is replaced or filtered per hour. CFM tells you what the equipment is moving. ACH tells you what that airflow means for the specific room.
Can a negative air machine increase air changes per hour?
A negative air machine can support higher air change rates when properly sized and configured for the space. The key is matching the machine’s effective CFM to the room volume and target ACH. Teams should also consider filtration, pressure relationships, ducting, and the specific infection control plan.
Do HEPA air purifiers count toward air changes per hour?
Portable HEPA filtration may contribute to equivalent or supplemental air cleaning depending on the application, setup, and facility policy. In healthcare settings, teams should confirm how portable filtration is treated under applicable standards, engineering guidance, and infection prevention requirements.
How many air changes per hour does an operating room need?
ASHRAE 170 requirements are commonly used for healthcare ventilation planning, and ASHE notes that operating rooms require a minimum of 20 air changes per hour under ASHRAE 170. Facilities should confirm the applicable edition, local code, AHJ interpretation, and room classification before making decisions.
The Real Business Case: Protect the Schedule Before the Delay Starts
The cost of lagging air changes is not only the cost of air movement. It is the cost of uncertainty inside a schedule that has very little room for uncertainty.

For an ASC, the strongest economic case is simple:
- Fewer delays protect room utilization
- Faster verification protects turnover time
- Better planning protects surgeon confidence
- Stronger containment and airflow control protect patient safety
- Clear documentation protects compliance confidence
- Consistent execution protects daily revenue
This is where the financial and clinical sides of the decision meet. The ASC does not need airflow calculations because the math is interesting. It needs them because the room cannot sit idle while teams debate whether the air is ready.
When construction, renovation, maintenance, or containment work touches an active surgical schedule, air changes should be calculated before they become a bottleneck.
Use the HEPACART® Air Change Calculator to estimate ACH, compare CFM to room volume, and plan air control with fewer last-minute surprises: Calculate Air Changes Per Hour

Share this
